Sunnyvale School District (SSD) and AT&T are proposing that a 65 foot tall Cell Phone Tower be built on the school grounds of Sunnyvale Middle School (SMS).
I think it is immoral and irresponsible to sell out the students and the school to for-profit corporations.
This is my flyer #1. Feel free to distribute this flyer, physically or electronically. I invite you to send me your design of a flyer. I will add to this blog so that people can print and distribute.
Picture of Uncle Sam downloaded from the internet. Believed to be circa 1917-1918. Use here is non-commercial.
If the Sunnyvale School Superintendent is deliberately suppressing the notification through the faculty, how do we get news to the students and families? PTA Mission: The overall purpose of PTA, according to National PTA.org:
- A powerful voice for all children
- A relevant resource for families and communities
- A strong advocate for the education and well-being of every child
PTA Values: What PTA stands for:
- Collaboration: We work in partnership with a wide array of individuals and organizations to accomplish our agreed-upon goals.
- Commitment: We are dedicated to promoting children’s health, well-being, and educational success through strong parent, family, and community involvement.
- Accountability: We acknowledge our obligations. We deliver on our promises.
- Respect: We value our colleagues and ourselves. We expect the same high quality of effort and thought from ourselves as we do from others.
- Inclusivity: We invite the stranger and welcome the newcomer. We value and seek input from as wide a spectrum of viewpoints and experiences as possible.
- Integrity: We act consistently with our beliefs. When we err, we acknowledge the mistake and seek to make amends.
According to these guidelines of the National PTA, even though the presidents and chairs of various PTAs may value money generated by the AT&T CPT lease, these PTAs still have the obligation to notify all parents and families of their schools, based on, especially, Mission Statement #2 Relevant Resource and Values Statement #5 Inclusivity.
It just pisses me off that these PTAs are also trying to prevent the spread of the notification just because they have the power to control the email lists. This is against everything a PTA stands for!
Here is an incomplete list of who is who at the PTAs of SMS and its feeder schools.
Other than the residents who live within 1/2 mile of 951 W. Remington Dr, who should care whether the AT&T Cell Phone Tower at Sunnyvale Middle School is approved?
Why? The teachers, the families and the students of Sunnyvale Middle School, of course.
Then, why haven't I heard single peep from SMS? This is sad indeed. I would like to believe that the Sunnyvale School Superintendent's office did such a good job suppressing the notification process that nobody knows. If you know anyone attending or will be attending SMS or any of the feeder schools listed below, please let them and their families know.
If the parents don't know, they can't get involved!
According to Sunnyvale School District website, SMS's feeder schools are Cherry Chase, Cumberland, Ellis and Vargas. And the boundaries for these feeder schools are:
But why the schools and town-owned properties such as parks?
Budgets are almost never, ever cut. No matter what anyone tells you that how hard the whole nation or world is doing a budget cut, budget cuts are almost never, ever successful. People simply cannot agree to cut their own pay. There are always reasons for not cutting this and that. People simply cannot agree to cut spendings, especially in their own department.
So more money has to come in from somewhere. And money with minimal work is most welcome.
Schools are the easiest target, especially in the economic downturns.
We cut number of teachers. We increase the number of students in class. We reduce the after school activities. But the higher up, the so-called support network bureaucrats are never reduced. In fact, if you dig deep enough, they probably have automatic pay raises like the senate and congress.
Parents are concerned that their children are not getting the competitive edge and attention at school if there are too many kids in a class. Parents are worried about having to pay for school after having to pay taxes that supposedly support the school system. Parcel tax? Direct drives?
So, if the FCC says its safe, who are we to argue about free money?
The School Board and the City Council are in with cell phone operators and tower builders for the money. The people who are supposedly working for us are falling for CPT builders' plot to deploy as many CPTs as possible during this economic crunch. These builders don't even have to build them now. Once approved, these CPTs and approvals will be "grandfathered" even if the FCC changes its ruling tomorrow. Therefore, these CPT builders are seeking out sites even though there is no need for them today.
Sunnyvale is not rich. But it is not poor. It is a working class city. It should be a city that can stand on its own feet. Not a city that would risk the children's future in return for money. It is despicable for the School Board and City Council to approve of CPTs in schools.
How can we hold these people accountable for their decisions? As with leaded gasoline case, effects of CPTs will be slow, "very slow gestation of that toxicological syndrome". It is impossible to hold these people accountable.
Schools and parks are easy targets because nobody is looking. Schools and parks are so-called transient properties. Nobody lives in them. Nobody needs to be notified according to FCC regulations. These properties are owned by a town and ran with money from taxes. One can say nobody owns these properties. One can also argue that every resident of Sunnyvale owns these properties.
If you want cell phones, you will have to accept Cell Phone Towers. But err on the safe side, put the CPTs somewhere else, away from schools, parks and places where children gather.
Don't let those making the decisions get away with being irresponsible. Use your voice as the people of Sunnyvale.
Sign the petition.
Go to the protest. Children are welcome.
Stay tuned for these coming events, get involved in your local groups, or do it yourself. Do something!
A German study looking at health records from 1994 - 2004, of 1000 patients showed higher incidents of health issues within 400 meters (1312 feet) of a CPT which was in operation since 1993. This research was done without external fundings.
By contrast, FCC's regulations were adopted in 1996.
In light of new research findings of health issues, isn't time for FCC to re-evaluated its policy on allowing CPTs to be sited on school grounds and in residential area?
If you would like to join a local yahoo group so that you can meet some of the people in the community to discuss the AT&T cell tower face to face, please go to:
This group may come in handy when it is time to organize the petition and protest.
This blog is not related to the yahoo group. This blog will not organize petitions or protests. If needed, this blog can be used to forward petitions to people who email their requests. This blog can also be used to communicate and broadcast protest events.
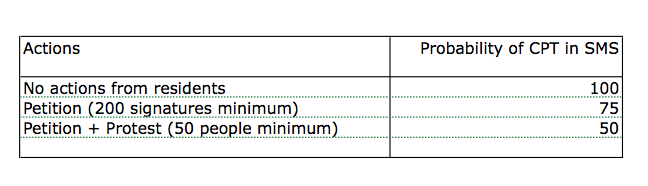
After my post last night, I received some emails asking me why I didn't think the CPT at SMS could be killed. Why I only gave the petition and protest 50% chance of killing AT&T's tower.
The main reason is that the Sunnyvale School District and the City Council want the money and have practically signed on the dots.
The only way to get to 100% chance of killing the AT&T tower is to get both the teachers and the students involved as well.
Without the teachers, the school comes to a halt. How many substitute teachers do you think the school keeps? Teachers have rights too. Just as International Association of Fire Fighters which opposes the use of fire stations as base stations, teachers and their association (California Teachers Association) can choose to oppose CPTs being built too close to school. After all, teachers spend more time at school than the students.
Teachers in SMS need to sign the petition to oppose the CPT. But teachers also have to be careful that the school and school district don't discriminate them for having voiced their opposition. Teachers need to keep a record of their performance evaluations and their students' appreciation of their work just in case the bureaucrats decide to cause trouble. Teachers who are not afraid to speak their opinions and to speak up for themselves are good examples to the students.
Students in SMS need to create and sign their own petition to oppose the CPT.
In the extreme case, for example, if the tower is approved but the students want to reverse the city's decision, as a last resort, students can choose to not attend school for a day or two. School districts get majority of the funding per student based on Average Daily Attendance (ADA). This funding roughly comes up to between $35-$45 per student per day (depending on the district). It will be also interesting to see how the school district explain the mass absence to the California Department of Education.
Those in power run their operations using fear tactics. Teachers who speak up might lose their jobs or affect their reviews. When teachers are forced to suppress their opinions and forbidden to discuss sensitive issues, students learn to be followers instead of people who dare to have a voice and question the stupidity of certain authorities.
How is America going to progress without people who are willing to challenge the status quo?
Now, the population of the US is about 308 million. That means only 1 out of 10 people doesn't carry a cell phone? Many people have multiple cell phones, for work, personal etc. But even young children are starting to carry cell phones because perhaps it gives the parents the peace of mind knowing they can reach their children any time and anywhere.
Almost 20% of homes in the US don't have land-lines anymore. With an additional 14% using cell phones almost exclusively even with land-lines at home. (cdc.gov 2009)
Number of cell phone subscriptions is not the only thing to consider in the economics of cell phones.
How much do people pay for their cellular subscriptions?
According to The Nielsen Company, average monthly cell phone bill is about $78 in 2009.
Do the math, 285 million cell phones in the US, multiply by $78 by 12 month: that is about $267 billion just on cell phone subscriptions alone.
Note: A projection from 2006 TIA press release claims that "total spending on wireless services is expected to reach $180.4 billion in 2009". (see TIA)
Even with the current economic problems, cell phone subscriptions continue to grow. Revenue for cell phone operators continue to rise. Demands for coverage and bandwidth continue to increase.
In short, people would rather cut their spendings on food than to reduce their cell phone usage, by going with a cheaper plan etc.
Demand is the first reason why Cell Phone Towers are sprouting up everywhere.
Cell Phone Towers are big money business. Two major CPT owners are American Tower and Crown Castle.
According to an inside source at American Tower, not all CPTs are created equal; a well-located CPT could fetch well over $300K in revenue per year.
The global addressable market for cell tower lease revenue is over $81.5 billion per year. The challenge is that most of this opportunity is not capitalized since mobile operators in most countries own and manage their own cell towers. Some partake in cell site sharing to reduce costs, but the model of third-party management is not widely implemented. The U.S. and Indian markets are the two markets where this opportunity hasn't gone un-noticed and third-party companies manage operator's passive infrastructure. In the U.S., cell tower operators like American Tower Corp. and Crown Castle International Corp. managed and/or operated approximately 30% of the over 260,000 cell sites in operation in the United States in 2009. The remaining sites are operator owned and managed or managed by property owners.
In North America, the total opportunity for cell-site leased revenue is $17.86 billion based on 2009 cell site numbers and average revenue per site. This does not include the opportunities for engineering firms to construct or augment existing towers. Only about 21% of this opportunity was realized in 2009. The average revenue per cell tower is $64,150 and average tenancy ratio is about 2.7.
Even in this recession, cell site business is booming as operators are forced to add new sites to reduce churn and remain competitive. For example America Tower has added 1,300 sites since the third quarter of 2008 and Crown Castle saw a 38% increase in tenant applications and a 12% site rental revenue increase.
For North America, most of the new growth will be in the coastal markets such as New York, Seattle, Los Angeles, Boston and San Francisco. There are also a lot of opportunities in Canada where Telus Mobility and Bell Mobility are launching HSPA networks that require new towers. In addition, a new mobile operator, Globalive Communications Corp. was set to enter the market and began building out a HSPA network, also requiring new cell sites. In the United States the following activities are talking place which will positively impact cell tower deployments:
• New towers are required by companies such as Clearwire Corp. which plans to deploy about 20,000 cell sites and is already leasing over 12,000 sites;
• Verizon Wireless and MetroPCS Communications Inc. are both planning LTE launches for 2010 and although the companies are planning to re-use existing sites, new tower construction may be required or augmentation to existing sites;
• AT&T Mobility will add more sites due to capacity constraints in its current 3.5G network;
• Cox Communications Inc. is building a new CDMA network in the AWS band;
• Sprint Nextel Corp. will have some growth.
The North American cell tower market remains strong even in one of the worst recessions seen since the Great Depression.
Profitis the second reason why Cell Phone Towers are sprouting up everywhere.
If you want cell phones, you will have to accept Cell Phone Towers, even if they are in your backyard.
But err on the safe side, put the CPTs somewhere else, away from schools, parks and places where children gather.
Those who don't want to see a CPT within SMS school grounds need to act NOW!
FCC has a new ruling in Nov 2009 to speed up the application and approval of Cell Phone Towers. See DOC-294711A1.
Excerpt:
Washington, D.C. – In a Declaratory Ruling (“Ruling”) adopted today, the Federal Communications Commission (“FCC”) cleared the way for broadband deployment by establishing timeframes of 90 days for collocations and 150 days for all other tower siting applications reviewed by state and local governments. This action will assist in speeding the deployment of next generation wireless networks while respecting the legitimate concerns of local authorities and preserving local control over zoning and land use policies.
This is AT&T's application to FCC. Reg # 1275578 filed 8/19/2010.
What is the probability that this CPT will be built?
This is just my pessimistic estimation. Obviously the more noise you make the better. The more times you knock on the city council member's door and the bigger your group the better your chance of getting the CPT killed.
"And in this sort of race, there's no silver medal for finishing second."
Tower accidents may be uncommon but cannot be ignored especially with the recent explosion of CPTs. Statistically speaking, we'll see more tower accidents.
According to City of Sunnyvale's Associate Planner Noren Caliva, the city will receive in the order of $25K per year from AT&T for the use of the land on SMS grounds to site the 65 foot tall Cell Phone Tower.
Lets look at the 3 most important questions about the money issue in this case:
1. Isn't $25K a lot of money?
2. Isn't this free money that AT&T is giving SMS?
3. Can we raise $25K on our own if we turn AT&T down? How?
1. Isn't $25K a lot of money?
First of all, $25K can be a lot of money depending how you look at it. Everything is a matter of perspective. What can $25K buy?
1. 15 new iMac computers, or
2. 65% of a teacher with 1-4 years of experience ($38K per year according to payscale.com),
3. infrastructural and technology improvements for the school,
4. PTA sponsored after school programs.
The real questions to ask are:
A. Is this money taxable? How much is left after tax?
B. How much of the money goes to SMS? How much goes to the whole school district?
C. What control SMS has over the money?
D. How much of this money will go to PTA to be spent directly on the students?
I suspect that the Sunnyvale School District will divvy up the money among other schools in the district. Not all schools are in the same financial state. SMS, Cumberland and Cherry Chase are in better shape than other schools in the SSD. These schools have great parent participation and the parents have always found ways to support after school programs with money from walkathons and direct drives. The same unfortunately cannot be said for the other schools in the district.
If you were the Superintendent, what would you do, when your job is to show that your district has great schools and great test scores? Would you let a few schools go way ahead of the others? Sooner or later, the SSD will say SMS is getting this extra $25K compared to other schools, so SMS should get less funding for years to come.
There are precedence that the schools are not getting the whole of the lease money from companies.
If the money does not go directly to the PTA or the school, which in this case will have to go through the city, the school or the PTA will have no say in where the money will go, if the money does come at all. It might even go to the pay increase of the Superintendent and school district office for all we know. It might be upgrading infrastructures that we don't need, etc. (We all know that there are funny businesses in all school districts and organizations which is why the budget and financial reports are so hard to locate.) There will be little control over how the money is spent within SMS. The PTA may even be told to still raise all the money it needs.
2. Isn't this free money that AT&T is giving SMS?
Nothing is free in this world.
By paying $25K a year, AT&T gets 35'x15' area of the school ground to put its tower and equipment plus easement access.
$25K divided by (35'x15') == $48 per square foot.
Wow, what a bargain compared to renting antenna space from Crown Castle's Cell Phone Tower at South Bernardo Drive live Verizon and others!! And AT&T will be able to increase its power at will and charge other carriers who want to have a piece of the tower. Perhaps this is what the AT&T rep means by "anticipating the future". A win-win situation without a doubt.
On the other hand, it is a lose-lose situation for SMS.
A. SMS students and faculty become Lab Rats for the radiofrequency emission from the tower as we all know and have concerns about.
B. Noise and other distractions cause by AT&T constructions and maintenance. There will be more than just the 525 square feet being used while these are underway.
C. Security issues. With the easement, AT&T can come and go as it desires. Now when the teachers and students and even the good neighbors see people loitering around the school campus in that area, they can no longer call the police department to check these people out. What is stopping people from wearing AT&T uniforms (do they even wear uniforms or do they only have badges?) and breaching our school grounds?
Schools are second homes to children. Children must be safe and feel safe when they are at school. The school, school district, city council members and all those making decisions have to be responsible for our children when they are in the school grounds.
3. Can we raise $25K on our own if we turn AT&T down? How?
Forget parcel tax, Cell Phone Towers and all the proposals done by the city. Only a fraction of the money will be seen within the schools.
A. Be self-sufficient and be 100% in control of SMS PTA's money:
$25K divide by 1000 (students in SMS) == $30 per family (assuming some multiple children families).
At the beginning of the school year, collect $30 from each family (or maybe $10 per additional child). What is $30 per family?
i) less than 1 month cell phone service, or
ii) less than 1 dinner out, or
iii) 1 new shirt, 1 pair of new pants, or
iv) 1 pair of new shoes, or
v) 1 DS game
B. Ask for corporate sponsors:
Write to Cisco, Facebook, Google, Intel, etc and explain the situation to them. I bet you they will come running to sponsor the school without asking for anything in return! It is great publicity for them to "save the school from being invaded by Cell Phone Towers". In return SMS can print the corporate logo on a small part of the shirts. Now, this is as close to free money as one can get!
Do we really want to find out that FCC is as wrong as the surgeon generals who had allowed leaded gasoline to be sold for more than 50 years? (About Lead Poisoning)
For the sake of our children's health and safety, don't let $25K per year make you turn a blind eye to AT&T's Cell Phone Tower.
We all want the best for our children. There are other ways to raise the money. Yes, it requires sacrifices. But these sacrifices are small compared to risking our children for our own greed for money and cell phone coverage.
Let us err on the precautionary side. As we always tell our children, "measure twice, cut once".
Lead interferes with a variety of body processes and is toxic to many organs and tissues including the heart, bones, intestines, kidneys, and reproductive and nervous systems. It interferes with the development of the nervous system and is therefore particularly toxic to children, causing potentially permanent learning and behavior disorders. Symptoms include abdominal pain, headache, anemia, irritability, and in severe cases seizures, coma, and death.
Routes of exposure to lead include contaminated air, water, soil, food, and consumer products.
Historically, approaches to lead-based paint have been reactive — responding to a lead-poisoned child — rather than the current preventive focus. Further, they focused on the ingestion of paint chips, ignoring lead-contaminated dust and soil.
While some cities enacted legislation on lead-based paint as early as the 1950s, it was not until 1971 that there was national legislation. During this period, there was little understanding about the effects of lead dust.
TITLE X (TITLE TEN) OF THE HOUSING AND COMMUNITY DEVELOPMENT ACT OF 1992
--> Title X represents a new strategy to reduce lead-based paint hazards that affects all HUD and other Federal housing programs. Some of the key features of Title X are that it:
----> Emphasizes the prevention of lead-based paint hazards before children are poisoned;
Lead in Gasoline:
After 15 workers in refineries died or lost their minds in 1924, it took EPA another 50 years to get lead additives out of gasoline. During this time, leaded fumes had gotten into our air, water and soil.
One most disturbing paragraph in the following paper:
"It should be emphasized, however, that scientific evidence capable of documenting this conclusion did not exist in previous decades. Only very recently have scientists been able to prove that low-level lead exposure resulting from automobile emissions is harmful to human health in general, but especially to the health of children and pregnant women."
Telecommunication industry is perhaps more powerful and has more money than automobil and oil industries of the past.
Romans of yesteryear, like Americans of today, equated limited exposure to lead with limited risk. What they did not realize was that their everyday low-level exposure to the metal rendered them vulnerable to chronic lead poisoning, even while it spared them the full horrors of acute lead poisoning.
The result, according to many modern scholars, was the death by slow poisoning of the greatest empire the world has ever known.
Then in December 1921, three General Motors engineers -- Charles Kettering, Thomas Midgeley, and Thomas Boyd -- reported tremendous success with their first test of tetraethyl lead. Through the Ethyl corporation, then a GM subsidiary, GM quickly began touting this lead compound as the virtual savior of the American automobile industry.
The discovery was indeed extremely important. It paved the way for the development of the high-power, high-compression internal combustion engines that were to win World War II and dominate the U.S. automotive industry until the early 1970s.
The deadliness of tetraethyl lead was sadly confirmed in the summer of 1924. Workers engaged in producing the additive fell sick and died at several refineries in New Jersey and Ohio. Banner headlines greeted each new fatality until a total of 15 workers had lost their lives -- and their minds.
In May 1925, the Surgeon General temporarily suspended the production and sale of leaded gasoline. He appointed a panel of experts to investigate the recent fatalities that had "occurred in the manufacture and mixing of the concentrated tetraethyl lead." The panel was also asked to weigh "the possible danger" that might arise "from...wide distribution of a lead compound" through its sale as a gasoline additive.
Industry dominated the Surgeon General's investigatory committee, which included only one genuine environmental visionary, Dr. Alice Hamilton of Harvard University. The Coolidge Administration gave the panel just seven months to design, run, and analyze its tests.
The committee's final report, published in June 1926, complained of the time constraints under which it had been forced to operate. Seven months was "not sufficient," argued the panel, "to produce detectable symptoms of lead poisoning" in experimental subjects because of the very slow gestation of that toxicological syndrome.
Nevertheless, the Surgeon General's panel ruled that there were "no good grounds for prohibiting the use of ethyl gasoline...as a motor fuel, provided that its distribution and use are controlled by proper regulations." The coming decades of Depression, total war, and post-war boom were hardly conducive to the implementation of "proper regulations" for leaded gasoline. Indeed, no compulsory standards were set for the industry until the early 1970s when EPA began its long, hard struggle to phase down lead levels in U.S. gasoline.
One saturnine prophecy marred the otherwise sanguine 1926 report to the Surgeon General. By 1985 these words were to reverberate with particular resonance down the corridors of time:
"It remains possible that, if the use of leaded gasolines becomes widespread, conditions may arise very different from those studied by us which would render its use more of a hazard than would appear to be the case from this investigation. Longer experience may show that even such slight storage of lead as was observed [among human guinea pigs] in these [1925] studies may lead eventually to recognizable lead poisoning or to chronic degenerative diseases of a less obvious character. In view of such possibilities the committee feels that the investigation begun under their direction must not be allowed to lapse.... With the experience obtained and the exact methods now available, it should be possible to follow closely the outcome of a more extended use of this fuel and to determine whether or not it may constitute a menace to the health of the general public after prolonged use or under conditions not now foreseen.... The vast increase in the number of automobiles throughout the country makes the study of all such questions a matter of real importance from the standpoint of public health."
Needless to say, this advice fell on deaf ears during the gin-soaked, jazz-crazed Roaring Twenties.
In 1927 the Surgeon General set a voluntary standard for the oil industry to follow in mixing tetraethyl lead with gasoline. This standard -- 3 cubic centimeters per gallon (cc/g) -- corresponded to the maximum then in use among refiners, and thus imposed no real restraint. Even without prodding, however, the industry did take giant strides toward instituting safer working conditions in oil refineries, thereby protecting individual laborers in the microcosm of the workplace.
Three decades later, the Surgeon General actually raised the lead standard to 4 cc/g (equivalent of 4.23 grams per gallon). This voluntary standard once again represented the outside range of industry practice. Nevertheless, the Surgeon General concluded in 1958 that a loosening of the voluntary standard posed no threat to the health of the average American: "During the past 11 years, during which the greatest expansion of tetraethyl lead has occurred, there has been no sign that the average individual in the U.S. has sustained any measurable increase in the concentration of lead in his blood or in the daily output of lead in his urine."
The actual industry average during the 1950s and the 1960s hovered in the vicinity of 2.4 grams per total gallon. The Department of Health, Education and Welfare (HEW), which was home to the Surgeon General starting with the Kennedy Administration, had authority over lead emissions under the Clean Air Act of 1963. The criteria mandated by this statute were still in the draft stage when the Act was reauthorized in 1970 and a new agency called EPA came into existence.
By then, the adverse effects of America's decades-old addiction to fossil fuel in general and leaded fuel in particular were becoming obvious to all. In January 1971, EPA's first Administrator, William D. Ruckelshaus, declared that "an extensive body of information exists which indicates that the addition of alkyl lead to gasoline...results in lead particles that pose a threat to public health."
It should be emphasized, however, that scientific evidence capable of documenting this conclusion did not exist in previous decades. Only very recently have scientists been able to prove that low-level lead exposure resulting from automobile emissions is harmful to human health in general, but especially to the health of children and pregnant women.
EPA took an emphatic stand on the issue in its final health document on the subject, "EPA's Position on the Health Implications of Airborne Lead," which was released on November 28, 1973. This study confirmed what preliminary studies had already suggested: namely, that lead from automobile exhaust was posing a direct threat to public health. Under the Clean Air Amendments of 1970, that conclusion left EPA with no option but to control the use of lead as a fuel additive known to "endanger the public health or welfare."
The very next month, in December 1973, EPA issued regulations calling for a gradual reduction in the lead content of the total gasoline pool, which includes all grades of gasoline. The restrictions were scheduled to be implemented starting on January 1, 1975, and to extend over a five-year period. The average lead content of the total gasoline pool of each refinery was to be reduced from the level of approximately 2.0 grams per total gallon that prevailed in 1973 to a maximum of 0.5 grams per total gallon after January 1, 1979. Litigation was to postpone implementation of this phasedown for two years.
Thalidomide was sold in a number of countries across the world from 1957 until 1961 when it was withdrawn from the market after being found to be a cause of birth defects in what has been called "one of the biggest medical tragedies of modern times".
It is not known exactly how many worldwide victims of the drug there have been, although estimates range from 10,000 to 20,000.
In the late 1950s and early 1960s, more than 10,000 children in 46 countries were born with deformities such as phocomelia, as a consequence of thalidomide use. The Australian obstetrician William McBride and the German pediatrician Widukind Lenz suspected a link between birth defects and the drug, and this was proved by Lenz in 1961.
The impact in the United States was minimized when pharmacologist and M.D. Frances Oldham Kelsey refused Food and Drug Administration (FDA) approval for an application from the Richardson-Merrell company to market thalidomide, saying further studies were needed. And although thalidomide was never approved for sale in the United States, millions of tablets had been distributed to physicians during a clinical testing program. It was impossible to know how many pregnant women had been given the drug to help alleviate morning sickness or as a sedative.
In 1960, Kelsey was hired by the FDA in Washington, DC. At that time, she "was one of only seven full-time and four young part-time physicians reviewing drugs" for the FDA. One of her first assignments at the FDA, was to review application by Richardson Merrell for the drug thalidomide (under the tradename Kevadon) as a tranquiliser and painkiller with specific indications to prescribe the drug to pregnant women for morning sickness. Even though it had already been approved in Canada and over 20 European and African countries, she withheld approval for the drug, and requested further studies. Despite pressure from thalidomide's manufacturer, Kelsey persisted in requesting additional information to explain an English study that documented a nervous system side effect.
Kelsey's insistence that the drug should be fully tested prior to approval was dramatically vindicated when the births of deformed infants in Europe were linked to thalidomide ingestion by their mothers during pregnancy. Researchers discovered that the thalidomide crossed the placental barrier and caused serious birth defects in infants. She was hailed on the front page of The Washington Post as a heroine for averting a similar tragedy in the US. Morton Mintz, author of The Washington Post article, said "[Kelsey] prevented ... the birth of hundreds or indeed thousands of armless and legless children." The public outcry was swift and drug testing reforms were passed unanimously by Congress a few months later. The drug testing reforms required "stricter limits on the testing and distribution of new drugs" to avoid similar problems. The amendments also, for the first time, recognized that "effectiveness [should be] required to be established prior to marketing."
- Magda Havas, PhD - Associate Professor of Environmental & Resource Studies (Trent University
- Martin Blank, PhD - Associate Professor of Physiology & Cellular Biology (Columbia University):
This is one of the most widely referenced papers. It is also the first hit on search engines for search of "children electromagnetics". Its conclusion is that exposure level from CPT (called mobile-phone base station in the paper) is too low to warrant any precautionary measures.
I think this is one of the most misleading paper I have ever read. Scroll down to see explanation and analysis.
Regarding the long-term health effects of mobile-phone use, the paucity of data, particularly for children, suggests that low- cost precautionary measures are appropriate, especially because some of the exposures are close to guideline limits. Physicians could advise parents that their children's RF exposure can be reduced by restricting the length of calls or by using hands-free devices to keep mobile phones away from the head and body. On the other hand, exposure levels from mobile-phone base stations are extremely low, and therefore precautionary measures do not need to be recommended.
I think the paper is misleading in many ways. In short:
It does a lot of "generally, it is believed..", "unlikely to..", "variations between children and adults, but..", "such studies have been uninformative..", "precautionary approach needed to cover the unknown cause-effect.."
And then BOOM:
It dismisses what it says and concludes that "exposure levels from mobile-phone base stations are extremely low, and therefore precautionary measures do not need to be recommended."
If you are patient enough to read the highlighted passage below, you will find that all throughout the paper, it talks about:
1. how children and adults differ physiologically, mainly central nervous system and brain
2. how children are more susceptible to EM radiations than adults even at small dosages
3. how epidemiologic studies show increase in childhood leukemia but not in laboratory studies
4. how direct studies on children are not widely done
5. how the physiological differences between children and adults make dosimetric calculations hard and perhaps inaccurate
6. how the paper's results and conclusions for children are based on dosimetric calculations and not through real measurement and clinical observations
7. how RF (mobile phone) radiations not as widely studied because of the rapid technology changes
8. "any increased sensitivity was considered to be covered by the more restrictive guidance on public exposure."
9. some effects are seen but are hard to reproduce because of varying methods and approaches
10. limited knowledge of the etiology of childhood leukemia and possibility of unknown cases but concludes unlikely RF Radiation.
11. hypotheses of disruption of the nocturnal production of melatonin in the pineal gland, subtle effects on melatonin physiology are not easily excluded, and such studies have not been conducted specifically on children 12. "SAR values and exposure variations for child models are similar to those for adults, although somewhat higher" (Similar and somewhat higer are totally different!) 13. "there is a need for dosimetric modeling of the distribution of SAR and temperature in children and also a requirement for appropriate age-related values for the dielectric properties of tissue."
14. then out of nowhere, it concludes that "exposure levels from mobile-phone base stations are extremely low, and therefore precautionary measures do not need to be recommended."
Does this sound suspicious to you?
I think this paper should raise more issues about how and why these researches are allowed to make such conclusions about EM Radiations on children than be quoted as evidence.
Abstract part on Page 2:
Exposure to electric and magnetic fields from 0 to 300 GHz has been increasing greatly as countries increase their capacity to generate and distribute electricity and take advantage of the many new technologies, such as telecommunications, to improve lifestyle and work efficiency (Fig 1). Evidence of an association between childhood leukemia and exposure to extremely low frequency (ELF) magnetic fields has led to their classification by the International Agency for Research on Cancer (IARC) as a "possible human carcinogen"1 based on consistent epidemiologic data and lack of support by laboratory studies in animals and cells. The reason why the results of the childhood leukemia studies are consistent is still being investigated, but one possibility is that children may be more sensitive to radiation in some or all parts of the electromagnetic spectrum.
Children's Susceptibility to Environmental Exposures on Page 4
Several aspects of exposure and susceptibility warrant a focus on children. In some exposure scenarios, children may receive higher doses than adults, resulting from higher intake and accumulation or differences in behavior. Greater susceptibility to some toxicants and physical agents has been demonstrated in children. Because the period from embryonic life to adolescence is characterized by growth and development, deleterious effects can occur at lower levels and be more severe or lead to effects that do not occur in adults; on the other hand, children can be more resilient because of better recuperative capacities.
Childhood Diseases Relevant to EMF Exposure on Page 5
Some diseases are limited to the embryo, child, or adolescent; other diseases that occur in children and adults manifest themselves differently in children. Of particular relevance to EMF exposure are childhood leukemia and brain cancer. There is consistent evidence from epidemiologic studies of a risk of childhood leukemia associated with exposure to environmentally high levels of ELF magnetic fields. There is no explanation for this effect from laboratory studies. An increased risk of brain cancer has been investigated in relation to ELF exposures and has been raised particularly in the context of mobile-phone use and the absorption of RF signals by the brain, although there is no convincing evidence suggesting an increased risk. To put potential EMF effects in perspective and determine how EMFs might be involved in the development of these diseases, we provide a brief overview of rates and risk factors for them.
on Page 5
As with most other cancers, the mechanism by which leukemia arises is likely to involve gene-environment interactions, the environmental exposures being derived from both endogenous and exogenous sources. Accordingly, it is important to identify exposures that either cause DNA damage and induce chromosome breaks that are repaired inadequately or act as promoters and/or progressers, ultimately leading to the overt expression of the disease. Exposures acting before birth and early in life have long been thought to be important determinants of leukemia; it is unfortunate that the evidence regarding the majority of suggested exposures is limited and often contradictory. Ionizing radiation given at large doses is one of the few known risk factors for leukemia.
on Page 6
RF fields are produced by radio and television broadcasts, mobile phones and base stations, and other communications infrastructure. Radio and television signals are broadcast to a large area from comparatively few sites. Mobile-phone base stations cover a smaller area and produce much lower emissions but are now much more common than radio and television stations (tens of thousands in many countries). Because of the width and angle of the RF signal beam and perturbation by the earth and building materials, there is little correlation between field strength and distance to the source. Typical power densities outdoors would be 0.01 to 1 mW · m–2 but could be orders of magnitude higher (ie, 100 mW · m–2 ). Depending on where the measurements are taken, base stations can be the largest individual source of RF fields, but other sources such as radio or television transmitters can result in comparable or greater exposures. Indoor levels are often lower by orders of magnitude, because buildings screen fields. A European median indoor power density of 0.005 mW · m–2 has been reported.
on Page 7
At present, population exposure to RF fields has been much less characterized than ELF fields, partly because of technical challenges (lack of adequate measuring equipment), the rapid evolution of mobile-phone technology (frequency, coding schemes), and new patterns of use (duration of calls, short-message services). However, the main reason ELF fields are better understood than RF fields is that they have been studied more.
on Page 7 and Page 8
Dosimetric calculations have not been conducted extensively for children and have not been undertaken for pregnant women and their unborn children. In general, adults exposed to ELF electric or magnetic fields have higher internal electric-field strengths and current densities than children because of size and shape differences. However, the distributions are different, and in children some tissues have higher field strengths and current densities for the same external field. Furthermore, children have significantly higher internal field strengths and current densities from contact currents than do adults. Dose computations using anatomically correct models of children30 reveal that modest, imperceptible current into the hand (10 μA) produces 50 mV · m–1 averaged across the lower-arm marrow of a small child and approximately 130 mV · m–1 in 5% of that tissue. During pregnancy, the magnitude and distribution of induced electric fields and currents in the mother will be different because of changes in body shape and will not have been assessed in the embryo or fetus. These factors, along with differences in dielectric properties, need to be taken into account in assessing health risks to children from ELF EMFs.
The guidance cited above was based on a consideration of laboratory evidence, including evidence from volunteer studies of magnetic phosphenes, and more recently on evidence from voltage-gated ion channel and neural-network behavior.29 Neurobehavioral studies in volunteers and in animals, mostly in adults, have not reported robust responses to ELF exposure31; overall, any changes seen have been subtle, transient, and reversible. Workshop participants thought that there is no reason to suppose a greater sensitivity of CNS neural networks and ion channels to induced electric fields in children or in the embryo or fetus. Reduced myelination seen in childhood and early adolescence was not thought likely to increase sensitivity either. It is not clear what the impact would be of an overabundance of synaptic connections seen in infants and early childhood, but any increased sensitivity was considered to be covered by the more restrictive guidance on public exposure.
Results from several independent research groups suggest that exposure to ELF magnetic fields at microtesla levels may disturb early development of bird embryos. However, replication attempts have been unsuccessful in some laboratories. Results from experiments with other nonmammalian experimental models (fish, sea urchins, and insects) have also suggested subtle effects on developmental stability.32 In mammals, prenatal exposure to ELF magnetic or electric fields does not result in strong adverse effects on development. Some effects of magnetic (or combined electric and magnetic) fields on postnatal development have been reported, but evaluation of the consistency of the findings is difficult because of the varying methods and approaches used in different studies.
on Page 8 and Page 9
An increased risk of childhood leukemia has been found to be consistently associated with exposure to environmental levels of power-frequency magnetic fields at levels very much below present guidance. Initial studies used a surrogate for magnetic fields (known as wire codes) that was based on distance and thickness of power lines near the residence.37 As instruments became available, the focus shifted to measured or calculated magnetic fields. Results of dozens of increasingly sophisticated studies and the 2 pooled analyses have reported a doubling of risk for children exposed to magnetic fields >0.3 to 0.4 μT compared with children exposed to fields <0.1 μT.38,39 Although a number of factors, including socioeconomic status, have been evaluated as confounders, substantial confounding has not been identified. However, because of limited knowledge of the etiology of childhood leukemia, it is difficult to exclude the possibility of some yet-to-be-identified confounder or of confounding by a combination of factors.Nevertheless, substantial confounding of the observed association, it seems to us, is unlikely. Although these results are also not likely to be a result of chance, bias cannot be ruled out.40 An epidemiologically detectable risk of leukemia for children, but not for adults, might result from either better exposure assessment for children or from greater susceptibility in children.
At present there is no experimental evidence that supports the view that this relationship is causal; however, few animal studies have been conducted using animal models of the predominant form of childhood leukemia, and most carcinogenesis bioassays begin when animals are sexually mature. In addition, there is no biophysical explanation for biologically significant interactions at these low field values, so if the association is causal, then there is currently no scientific explanation. Two hypotheses for such effects were discussed at the workshop.
One hypothesis discussed at the workshop proposed that the association of power-frequency magnetic fields with childhood leukemia may result from the flow of electric current through the bone marrow of children after contact with water fixtures or a water stream in which a small voltage difference exists as a result of the grounding of the residential electrical system to the water pipe.41 Calculation shows that potentially significant electric fields (more than 100 mV · m–1 ) may be induced in the bone marrow in these circumstances; this lends biological plausibility to the proposed mechanism. The effect of such weak electric fields in inducing effects in hematopoietic tissue that might increase the risk of ALL, possibly by affecting preleukemic clones (see above), has not been investigated.
A second hypothesis suggested that exposure to power-frequency magnetic fields increases the risk of childhood leukemia through disruption of the nocturnal production of melatonin in the pineal gland.42 Although the International Commission on Non-ionizing Radiation Protection43 concluded that there is no convincing evidence of an effect, subtle effects on melatonin physiology are not easily excluded, and such studies have not been conducted specifically on children.
Recommendations were made for additional research regarding the association between exposure to power-frequency magnetic fields and childhood leukemia; it is clear that this issue is unresolved. Although such scientific uncertainty remains, the WHO recommends the adoption of precautionary measures for the protection of children (see below).
Exposure to RF radiation induces heating in body tissues and imposes a heat load on the whole body; guidance on exposure is based on avoiding the risks to health that result from localized rises in tissue temperature and from the physiologic stress engendered by excessive whole-body heat loads.28,29 Present guidance on occupational exposure is based on restricting the RF-induced whole-body specific absorption rate (SAR) to <0.4 W · kg–1 , a heat load sufficiently small that its contribution to other possible heat loads, generated from hard physical work and/or imposed by high ambient temperatures, can be neglected. Basic restrictions on localized SARs, averaged over any 10 g of contiguous tissue, are 10 W · kg–1 in the head and trunk and 20 W · kg–1 in the limbs.28 These are intended to restrict local tissue temperature rises to acceptable levels.
Guidance on public exposure incorporates an additional safety factor of 5, reducing the basic restrictions to 0.08 W · kg–1 to the whole body and 2 W · kg–1 to the head. Temperatures are derived from dosimetric calculation and thermal modeling; SARs are also related to external field values via dosimetric calculation. The corresponding reference levels, which for RF fields are power densities, are frequency dependent and are of the order of 10 W · m–2 at 1800 MHz for general public exposure.
Dosimetric calculation has for more than a decade allowed for differences in body size between children and adults, and these differences have been factored into guidance. Despite large differences in the size, shape, and tissue distribution of heads, the SAR values and exposure variations for child models are similar to those for adults, although somewhat higher. In addition, the relative depth of penetration is larger for children, a logical consequence of smaller head diameter. Dielectric studies encompassing several tissue types, including brain, obtained from newborn to fully grown rats, mice, and rabbits exposed to RF EMF in the frequency ranges of 130 MHz to 10 GHz and 300 kHz to 300 MHz report large, age-related variations in the permittivity and conductivity of brain tissue and even larger variations for skin and skull tissue.44–46 Thus, there is a need for dosimetric modeling of the distribution of SAR and temperature in children and also a requirement for appropriate age-related values for the dielectric properties of tissue.
Many different nonthermal mechanisms for RF interaction with tissue have been considered in recent studies.48–50 These are not particular to children, but if any were confirmed at levels below current guidance, then questions might also be raised about potential childhood susceptibility. Possible RF electric-field interactions51 include (1) changes in the conformation of proteins, including ATPases associated with ion channels, resulting in functional changes in the proteins, (2) changes in the binding of ligands such as Ca2+ to cell receptor proteins, also resulting in changed receptor function, (3) absorption of RF energy by the vibrational states of biological components such as microtubules, (4) enhanced attraction between cells (the pearl-chain effect), and (5) demodulation of a modulated RF signal, producing ELF electric fields. Generally, it was considered that such interactions are unlikely to be biologically significant at RF levels below guidance values.
For infant, childhood, and adolescent exposure, the maturation of the CNS has been raised as potentially susceptible. In this context, the major changes to the CNS during this period comprise a maturation of the hard-wiring (namely, increased myelination), facilitating the transmission of information, which occurs rapidly over the first 2 years but extends into the second decade of life, and remodeling of the synaptic connections between neurons8 after the first 2 years and into adolescence, mostly by synapse elimination as redundant connections are lost. With regard to synaptogenesis, spontaneous and stimulus-evoked electrical activity in the CNS is believed to play a crucial role in local competition between growing nerve axons and the distribution of their synaptic boutons on target cells.52 Whether RF fields could affect these processes is not known. Neurobehavioral studies in volunteers and in animals, mostly adults, have not reported robust responses to RF exposure, particularly that associated with mobile phones.31
Numerous studies have evaluated developmental effects of RF fields on mammals, birds, and other nonmammalian species.53,54 These studies have shown clearly that RF fields are teratogenic at exposure levels that are high enough to cause significant increases in temperature. There is no consistent evidence of effects at nonthermal exposure levels, although only a few studies have evaluated possible effects on postnatal development using sensitive end points such as behavioral effects.
on Page 10
Several ecological studies59–66 have examined cancer risk, including risk of childhood leukemia, among populations living in proximity to radio and television broadcast towers. Often driven by a previously identified cluster, these analyses are based simply on distance from the source and often include an extremely small number of cases. Such studies have been uninformative. More rigorous investigations might be feasible with development of new instruments capable of capturing personal RF exposure.
Few relevant epidemiologic or laboratory studies have addressed the possible effects of RF exposure on children. Because of widespread use of mobile phones among children and adolescents and relatively high exposures to the brain, investigation of the potential effects of RF fields on the development of childhood brain tumors is warranted. The importance of longer lifetime exposure has been emphasized by a recent study67 in which acoustic neuroma occurred only after 10-year use of mobile phones. The type of mobile-phone use among children (eg, text messaging), their potential biological vulnerability, and longer lifetime exposure make extrapolation from adult studies problematic. Such scientific uncertainty can be addressed through both the application of precautionary policies and through additional research.
In today's world, technologic developments bring both social and economic benefits to large sections of society; however, the health consequences of these developments can be difficult to predict and manage. Nevertheless, even if the effects are small, a widespread exposure can have large public health consequences. When risks are complex, an established cause-effect relationship is absent, or the scientific findings are not robustly quantifiable, the need for timely preventive action makes a precautionary approach an essential part of policy making. Many societies believe that this is particularly true regarding children (including the unborn child): they represent the future of the society, have the potential for longer exposure than adults, and yet are less able to manage their own risk.
International guidance on occupational and public exposure to EMFs, described above, is based on avoiding risks to health that are well understood and for which there is good scientific evidence. However, with regard to childhood exposure to EMFs (and exposure during pregnancy), several factors argue for the adoption of precautionary measures, including the possibility that EMFs might affect children; the dread with which some of the diseases raised in this context, such as leukemia and
brain cancer, are perceived; the involuntary nature of some of the exposure; its extensiveness; and its likely rapid growth in the future.
The WHO International EMF Project (www.who.int/emf) is finalizing a practical framework for guiding policy options in areas of scientific uncertainty that is based on the application of precaution.68 In general terms, the draft WHO precautionary framework aims to develop a set of public health policy options that can be applied according to the degree of scientific uncertainty and the anticipated severity of the harm that might ensue from exposure, taking into account the size of the affected population and the cost of exposure reduction. These measures should not be seen as undermining science-based guidance on exposure; rather, they represent additional steps with application that may vary from country to country depending on social and economic considerations.
Precautionary measures may also be adopted at an individual level, depending on the degree of concern felt by the exposed person. In giving advice to their patients, physicians should weigh the strength of scientific evidence for the risk, if any, of an adverse outcome, the benefits of the technology, and the feasibility of reducing exposure, as well as the overall health of the patient, which includes freedom from worry and anxiety.
For ELF (power-frequency) fields, there is some evidence that exposure to environmental magnetic fields that are relatively high but well below guidance levels is associated with an increase in the risk of childhood leukemia, a very rare disease (even if the risk is doubled, it remains small at 5–8 per 100000 children per year). Although the evidence is regarded as insufficient to justify more restrictive limits on exposure, the possibility that exposure to ELF magnetic fields increases risk cannot be discounted. For the physician faced with questions from, for example, a couple planning a family and concerned about this issue, or from someone pregnant and occupationally exposed to relatively high ELF magnetic fields, standardized advice is not possible. Instead, physicians could inform their patients of possible risk and advise them to weigh all the advantages and disadvantages of the options available to them (of which EMF reduction is but one consideration). Some simple options include reducing exposure by minimizing the use of certain electrical appliances or changing work practices to increase distance from the source of exposure. People living near overhead power lines should be advised that such proximity is just an indicator of exposure and that homes far away from power lines can have similar or higher fields.
Regarding the long-term health effects of mobile-phone use, the paucity of data, particularly for children, suggests that low- cost precautionary measures are appropriate, especially because some of the exposures are close to guideline limits. Physicians could advise parents that their children's RF exposure can be reduced by restricting the length of calls or by using hands-free devices to keep mobile phones away from the head and body. On the other hand, exposure levels from mobile-phone base stations are extremely low, and therefore precautionary measures do not need to be recommended.
























{kind=link}